Citation: News of Beam Diagnostics Belarus 2000 1: 26-27.
Our experience with CT-angiography.
Rutskaja E. A.1, Kavetskij S. I.2
1Belarussian Medical Academy of Postgraduate Education, 2Republican
Scientific Clinical Center of Pediatric Oncology and Hematology, Minsk.
|
|
| Figure 1. Neck vessels CT-angiography of patient with laryngeal
cancer. Metastatic lymph nodes at the level of common carotid artery bifurcation
compressing internal jugular vein. Dilated collaterals in the system of
superficial jugular vein seen. |
|
|
|
| Figure 2. Ganglionevroma of upper mediastinum in 10 y. o. child.
(а)
Vessels in the background of tumour can’t be differentiated. |
|
|
|
| Figure 2. (b) As may be seen after IV contrast administration,
left subclavian artery is incorporated by tumour, left common carotid artery
moved forward. |
|
|
|
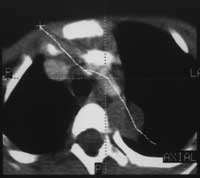
| Figure 2. The same patient. (c) Curved white line depicts
reformation plane. |
|
|
|
| Figure 2. (d) Resulting reformat along aorta arch demonstrates
vessels relation to tumour in different perspective. |
|
|
|
| Figure 3. CA-angiogram in patient with lung cancer demonstrates
filing defect in the lumen of main and left pulmonary arteries as signs
of tumour invasion. |
|
|
|
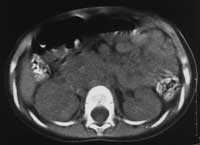
| Figure 4. Right adrenal nefroblastoma in 1,5 y. o. patient.
(а)
Native CT. |
|
|
|
| Figure 4. (b) CTA in the same patient. Vena cava inferior
compressed and incorporateb by the tumour. Blood collateral flow to vena
hemiazygos may be seen. |
|
|
|
| Figure 5. Right adrenal nefroblastoma in 6 y. o. patient. A-B,
C-D - tumour thrombus in the lumen of vena cava inferior. |
|